

Stern Electronics Pty. Ltd.
est. 1973 A.C.N 010695360
est. 1973 A.C.N 010695360


How can DVT be prevented
As DVT and PE can produce few symptoms and clinical diagnosis can be unreliable, often
the diagnosis cannot be established until a large Pulmonary Embolism (PE) has occurred
or until autopsy. As a result, the preferred approach is to prevent the onset of DVT and PE.
There are a number of prophylactic measures aimed at reducing the risk of DVT, including
pharmacological interventions and mechanical techniques such as graduated compression
stockings (GCS) and pneumatic compression devices (PCD) that reduce the risk of thrombosis
without causing haemorrhage.
the diagnosis cannot be established until a large Pulmonary Embolism (PE) has occurred
or until autopsy. As a result, the preferred approach is to prevent the onset of DVT and PE.
There are a number of prophylactic measures aimed at reducing the risk of DVT, including
pharmacological interventions and mechanical techniques such as graduated compression
stockings (GCS) and pneumatic compression devices (PCD) that reduce the risk of thrombosis
without causing haemorrhage.
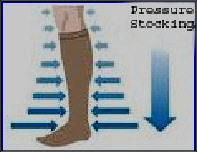
Graduated compression stockings (GCS)are the most widely used and lowest-cost DVT
prophylactic measure but the least effective. They are designed to produce a relatively high
pressure at the ankle with diminishing compression up the calf to the knee or above. GCS
work best in combination with other measures.
Sequential compression reduces the incidence of DVT and is more effective than graduated
compression stockings in high-risk patients in combination with anticoagulants or when
anticoagulants are contraindicated. It is estimated that sequential compression reduces the
risk of DVT by 60%. There are an increasing number of reports supporting CD efficacy in DVT
prevention in a range of clinical conditions. The reported incidence of DVT is up to 10% with
current CD.
Traditionally DVT prevention is only given during hospital stay. For high risk patients there is
growing recognition of the benefits of preventative measures applying before surgery and
continuing until the patient is fully ambulatory.
pressure at the ankle with diminishing compression up the calf to the knee or above. GCS
work best in combination with other measures.
Sequential compression reduces the incidence of DVT and is more effective than graduated
compression stockings in high-
risk of DVT by 60%. There are an increasing number of reports supporting CD efficacy in DVT
prevention in a range of clinical conditions. The reported incidence of DVT is up to 10% with
current CD.
Traditionally DVT prevention is only given during hospital stay. For high risk patients there is
growing recognition of the benefits of preventative measures applying before surgery and
continuing until the patient is fully ambulatory.

Pevention